Meiqi Wu1, Yanyu Wang2, Qiao Yang1, Xuezhu Wang1, Xu Yang2, Haiqun Xing1, Xinting Sang2, Xiang Li3, Haitao Zhao2, Li Huo4
Abstract
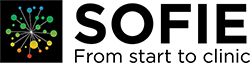
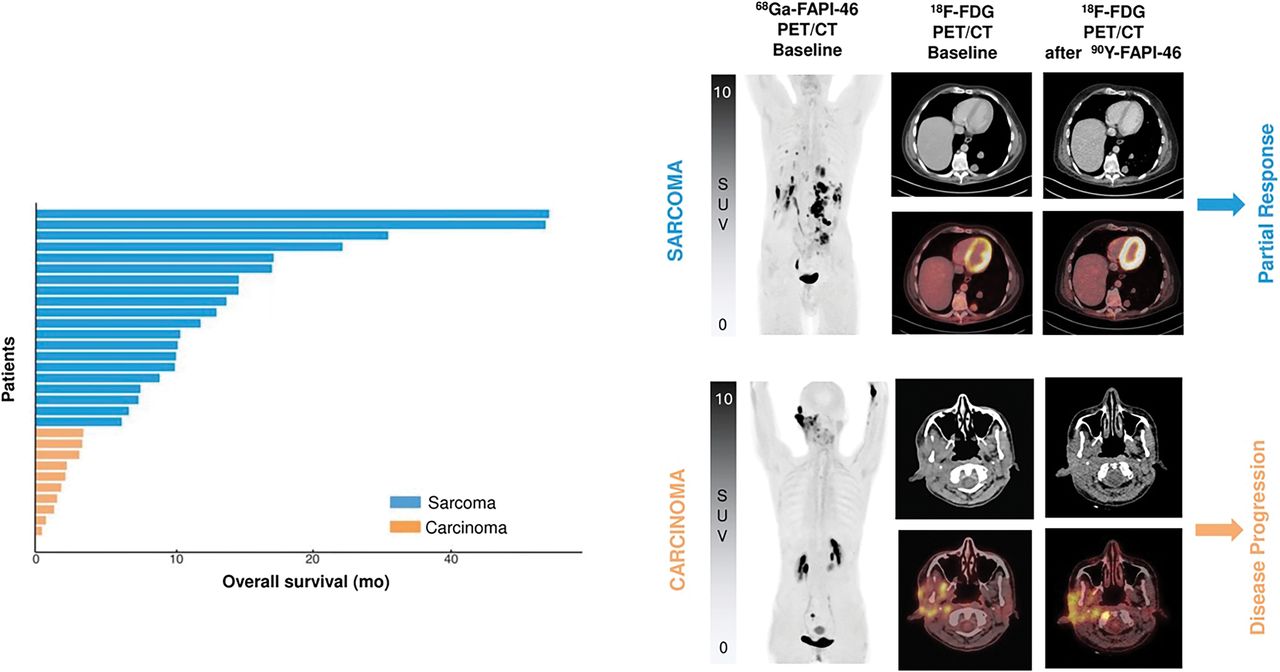
Fibroblast activation protein contributes to immunosuppression and resistance to immunotherapies. This study aimed to compare baseline 68Ga-labeled fibroblast activation protein inhibitor (68Ga-FAPI) PET/CT and 18F-FDG PET/CT in response and survival prediction in unresectable hepatocellular carcinoma (uHCC) patients treated with the combination of programmed cell death 1 (PD-1) inhibitor and lenvatinib. Methods: In this prospective cohort study, 22 patients with uHCC who underwent baseline 18F-FDG and 68Ga-FAPI PET/CT and soon began taking a combination of PD-1 inhibitor and lenvatinib were recruited. Semiquantitative indices of baseline PET/CT were measured as 18F-FDG SUVmax, metabolic tumor volume, total lesion glycolysis, 68Ga-FAPI SUVmax, 68Ga-FAPI-avid tumor volume (FTV), and total lesion fibroblast activation protein expression (TLF). The primary endpoint was durable or nondurable clinical benefit after treatment, and the secondary endpoints were progression-free survival (PFS) and overall survival (OS). Results: The overall response rate of the combination therapy was 41% (9/22). Fifty percent of patients had durable clinical benefit. Median PFS and OS were 4.8 and 14.4 mo, respectively. Patients with nondurable clinical benefit showed a significantly higher FTV and TLF than those with durable clinical benefit, whereas 18F-FDG parameters overlapped. A higher 68Ga-FAPI-avid tumor burden (FTV > 230.46 cm3 or TLF > 961.74 SUVbody weight⋅cm3) predicted both shorter PFS (4.0 vs. 13.5 mo, P = 0.016) and shorter OS (7.8 mo vs. not reached, P = 0.030). Patients with a higher metabolic tumor burden (metabolic tumor volume > 206.80 cm3 or total lesion glycolysis > 693.53 SUVbody weight⋅cm3) showed a shorter OS although the difference did not reach statistical significance (P = 0.085). In multivariate analysis, a higher 68Ga-FAPI-avid tumor burden (hazard ratio [HR], 3.88 [95% CI, 1.26-12.01]; P = 0.020) and macrovascular invasion (HR, 4.00 [95% CI, 1.06-15.14]; P = 0.039) independently predicted a shorter PFS, whereas a higher 68Ga-FAPI-avid tumor burden (HR, 5.92 [95% CI, 1.19-29.42]; P = 0.035) and bone metastases (HR, 5.88 [95% CI, 1.33-25.93]; P = 0.022) independently predicted a shorter OS. Conclusion: Volumetric indices on baseline 68Ga-FAPI PET/CT were potentially independent prognostic factors to predict durable clinical benefit, PFS, and OS in uHCC patients treated with a combination of PD-1 and lenvatinib. Baseline 68Ga-FAPI PET/CT may facilitate uHCC patient selection before combination therapy.
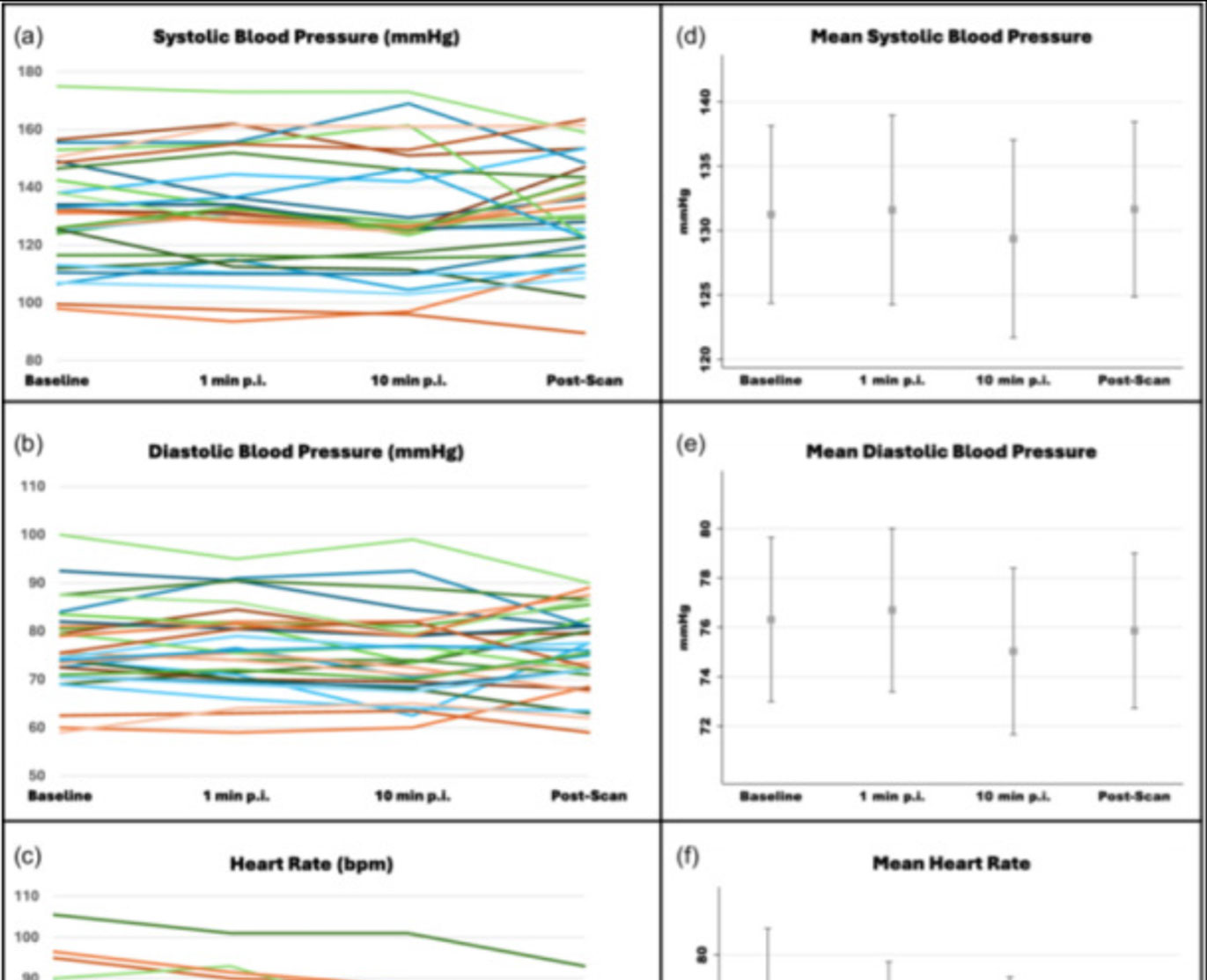
![Safety of [68Ga]Ga-FAPI-46 PET/CT including hemodynamic measurements and patient-reported outcomes in cancer patients](https://sofie.com/wp-content/uploads/2026/05/NewImage-500x383.jpg)
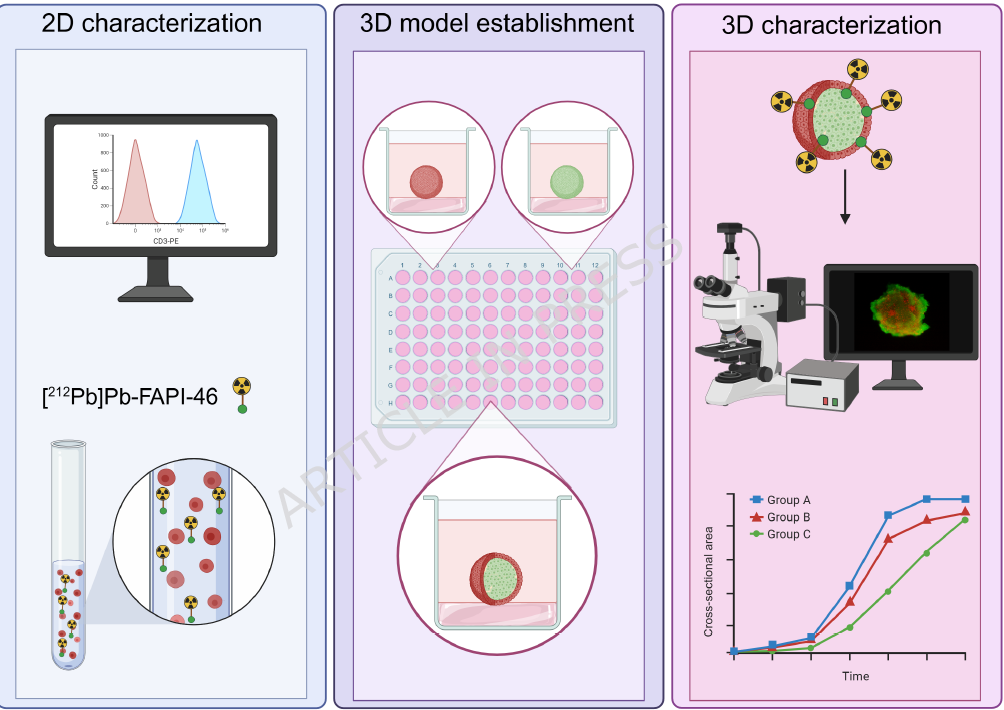
![A 3D co-culture model with fibroblast-restricted FAP expression for cancer therapy using [212Pb]Pb-FAPI-46](https://sofie.com/wp-content/uploads/2026/06/A-3D-co-culture-model-with-fibroblast-500x383.png)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}